Treatment Of Nephritic Syndrome
Nephritic syndrome often occurs secondarily as a consequence of systemic autoimmune diseases. However, it can also be due to both generalized and local infections.
Treatment of nephritic syndrome is intended to prevent serious life-threatening complications such as chronic glomerulonephritis and chronic kidney disease. In this sense, timely medical assistance will guarantee, to a great extent, the improvement of the patient.
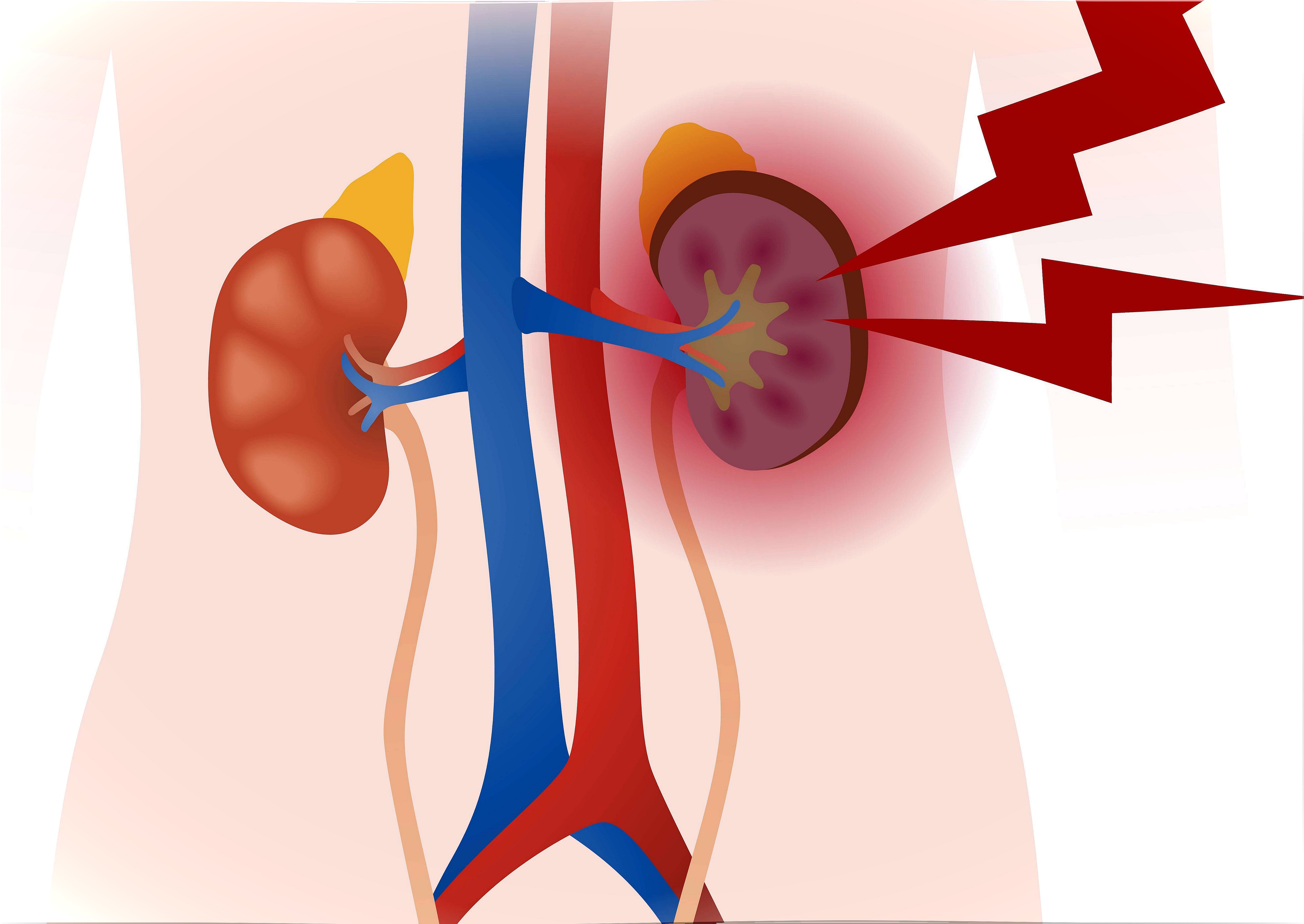
Symptoms caused by inflammation of the glomeruli are called nephritic syndrome. Gromeruli are kidney units that are responsible for the filtering process. This disease is characterized by the sudden onset of hematuria, oliguria, proteinuria, and edema. It is usually accompanied by kidney impairment and hypertension.
How does nephritic syndrome occur?
Nephritic syndrome occurs when injury occurs as a result of inflammation of the glomeruli of the kidney. This allows plasma proteins and blood cells to pass into the urine. As a result, blood clearance is reduced and urine production is significantly decreased with the risk of total absence of diuresis (anuria). This situation produces an accumulation of nitrogenous substances in the blood and, in addition, causes retention of water and salts (edema) and arterial hypertension.
Some Causes of Nephritic Syndrome
Infections
- Bacterial (due to streptococci, staphylococci or pneumococci).
- Viral (hepatitis B and C or HIV infection).
- Parasitic (for example, malaria).
- Fungal or mycosis.
Vasculitis or inflammation of the blood vessels
- Eosinophilic granulomatosis with polyangiitis.
- Granulomatosis with polyangiitis.
- Cryoglobulinemia.
Immune disorders
- Systemic lupus erythematosus (lupus).
- Goodpasture syndrome.
Other causes
- Hereditary nephritis.
Diagnosis
Doctors order tests to detect nephritic syndrome for symptoms of bleeding in the urine and fluid retention (edema). The diagnosis is confirmed by the results of laboratory tests that indicate kidney dysfunction and blood cells and protein in the urine.
If something more serious is suspected, a kidney biopsy is performed to confirm the diagnosis. This is done to determine the causes and extent of scar tissue. Also, to estimate the chances of reversing the damage.
Treatment of nephritic syndrome
There is no specific treatment to cure nephritic syndrome. However, depending on the severity of the symptoms and their cause, the doctor will suggest certain care and medications.
In any case, the main goal of treatment is to reduce inflammation, edema, and hypertension. If the kidneys are unable to cleanse the blood of toxins and residual fluids, dialysis may be required.
General care measures
In the acute phase, the treatment of nephritic syndrome is based mainly on rest. Regular reviews of body weight, blood pressure, and kidney and cardiovascular status are also made. To reduce symptoms and avoid complications, your doctor may suggest:
- Maintain a good daily water and dietary balance.
- A strict low sodium diet with fluid restriction.
- In renal failure and oliguria, phosphates and potassium should also be restricted.
- A low protein diet is advised.
Pharmacological measures

1. Antibiotics
In the treatment of nephritic syndrome, antibiotics will be given only if there is an active bacterial infection. The formula and dosage may vary depending on the patient, the cause and the level of severity. Typically, they are used:
- Oral penicillin G at a dose of 125 milligrams every 6 hours for 10 days or intramuscular benzathine penicillin (600,000 or 1,200,000 U, single dose).
- In allergic patients, erythromycin is used orally (125-250 milligrams every 6 hours) for 10 days.
2. Diuretics
Loop diuretics are administered when there is a clinical circulatory overload : edema or arterial hypertension. They are also indicated if signs of congestive heart failure are detected radiologically.
- The dose of furosemide is 0.5-2 mg / kg / day orally, for moderate cases.
- If there is a severe overload, the dose can be increased to 10 mg / kg / day.
3. Antihypertensives
If, despite improving diet and diuretics, blood pressure does not stabilize, antihypertensive drugs will be included in the treatment.
- Angiotensin converting enzyme inhibitors are not advised because they increase potassium levels.
- With vasodilator action such as hydralazine at a dose of 0.5-2 mg / kg / day orally.
- Calcium antagonists such as nifedipine 0.25-2 mg / kg / day, in 2 or 3 doses.
4. Vasodilators
For hypertensive crisis, hypertensive encephalopathy, and acute lung edema, hospitalization in an intensive care unit is required and vasodilators are administered.
- Alpha and beta blockers such as labetalol (1.3 mg / kg / h, intravenously, or 4 mg / kg / day in 1 or 2 doses, orally).
- Nitroprusside in intravenous infusion (0.5-8 μg / kg / min or 1-2 mg / kg / dose / h).
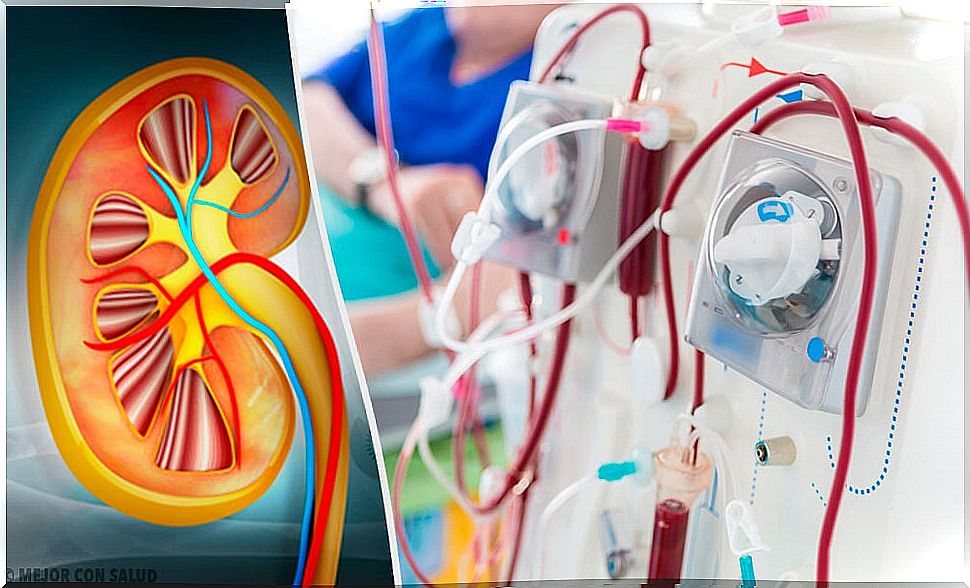
5. Dialysis, a treatment option for nephritic syndrome

A small number of patients with nephritic syndrome go on to require dialysis. It is usually done when the kidneys suffer damage that prevents them from working properly.
Depending on the case, the doctor may suggest peritoneal dialysis or hemodialysis.
Forecast
With timely intervention, most cases progress favorably. In a few days, an acceptable diuresis is restored. After two or three weeks, the edema, hypertension and hematuria disappear.
However, in certain cases, hematuria can persist for up to 2 years without causing complications or an unfavorable prognosis. Some of the complications that could occur are congestive heart failure (the most common), hypertensive encephalopathy, and acute kidney failure.